This will be your resource page leading up to the exam.
OSCE VIVA Meeting 1 |
ECGs for the Fellowship |
|
|
|
OSCE VIVA Meeting 2 1st August |
Homework before the 8th August VivaPrepare a standard AIRWAY answer for:
|
OSCE VIVA Meeting 8/8/22
|
|
|
|
Here is the PDF you can download, for teaching structure. Chapters 2 and 4 are the ones to concentrate on.
|
| ||
OSCE Viva Meeting 22 August
Predictions for 2022.2
Below you will find a PDF of Will's detailed predictions. Please review. There is also a single page of my predictions.
Please read the predictions and send us any questions you may have. Will and I will then put together a short video lecture answering your questions and put it up here on this page.
Please read the predictions and send us any questions you may have. Will and I will then put together a short video lecture answering your questions and put it up here on this page.
|
Will's detailed recommendations
|
Peter's last minute high chance topics
| ||
Here are some links to fracture Material
Elbow Fractures
Unstable Pelvic Fractures
Diagnosing Scaphoid Fractures
Gilula's Carpal Arcs
Elbow Fractures
Unstable Pelvic Fractures
Diagnosing Scaphoid Fractures
Gilula's Carpal Arcs
VIDEO Homework OSCEs with answers
QUESTION 1 + ANSWER
Candidate Instructions
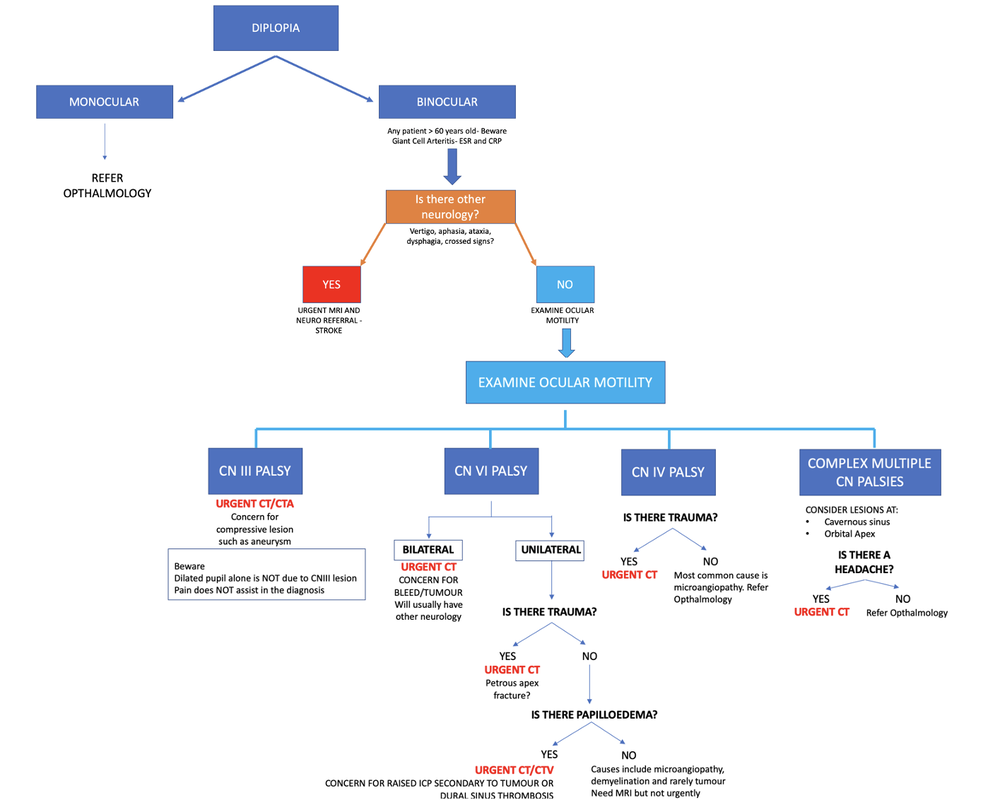
You are working in a rural emergency department and your registrar wishes to discuss a patient with you who has presented with diplopia.
This is a 54 yo male with a PMHx of hypercholesterolaemia and hypertension, both well controlled on medication, who has developed double vision over the last 2 hours.
He does not complain of any other neurology.
Please outline your approach to the examination of this patient.
You will be assessed on:
This OSCE Examines the DOMAINS of:
ANSWER
Questions to answer
•VA
•VF
•Pupils size and reactivity
•RAPD
•Monocular/Binocular
•View of retina- papilloedema
•Raised IOP- tumour or dural sinus thrombosis
•Extra ocular muscles
•CNIII
•pupil dilated
•Eye down and out and
•Partial ptosis
•Multiple CN- Cavernous sinus lesion
•Slit lamp
•?Pressures glaucoma
Examiner will prompt
•What are you looking for?
•Expect to discuss all findings
•VA
•VF if not intact could be a tumour or bleed
•Pupils- dilated pupil ? CNIII not if on own
•If trauma
•CN IV-
•CN VI- petrous apex fracture
•Headache- may be tumour specially if multiple CN involved
You are working in a rural emergency department and your registrar wishes to discuss a patient with you who has presented with diplopia.
This is a 54 yo male with a PMHx of hypercholesterolaemia and hypertension, both well controlled on medication, who has developed double vision over the last 2 hours.
He does not complain of any other neurology.
Please outline your approach to the examination of this patient.
You will be assessed on:
- Differential Diagnoses
- Description of Examination technique
- Identification of causes related to findings
This OSCE Examines the DOMAINS of:
- Medical expertise
ANSWER
Questions to answer
•VA
•VF
•Pupils size and reactivity
•RAPD
•Monocular/Binocular
•View of retina- papilloedema
•Raised IOP- tumour or dural sinus thrombosis
•Extra ocular muscles
•CNIII
•pupil dilated
•Eye down and out and
•Partial ptosis
•Multiple CN- Cavernous sinus lesion
•Slit lamp
•?Pressures glaucoma
Examiner will prompt
•What are you looking for?
•Expect to discuss all findings
•VA
•VF if not intact could be a tumour or bleed
•Pupils- dilated pupil ? CNIII not if on own
•If trauma
•CN IV-
•CN VI- petrous apex fracture
•Headache- may be tumour specially if multiple CN involved
QUESTION 2 + ANSWER
CANDIDATE NOTES
You are at your tertiary referral hospital, it is 11 am on a Wednesday.
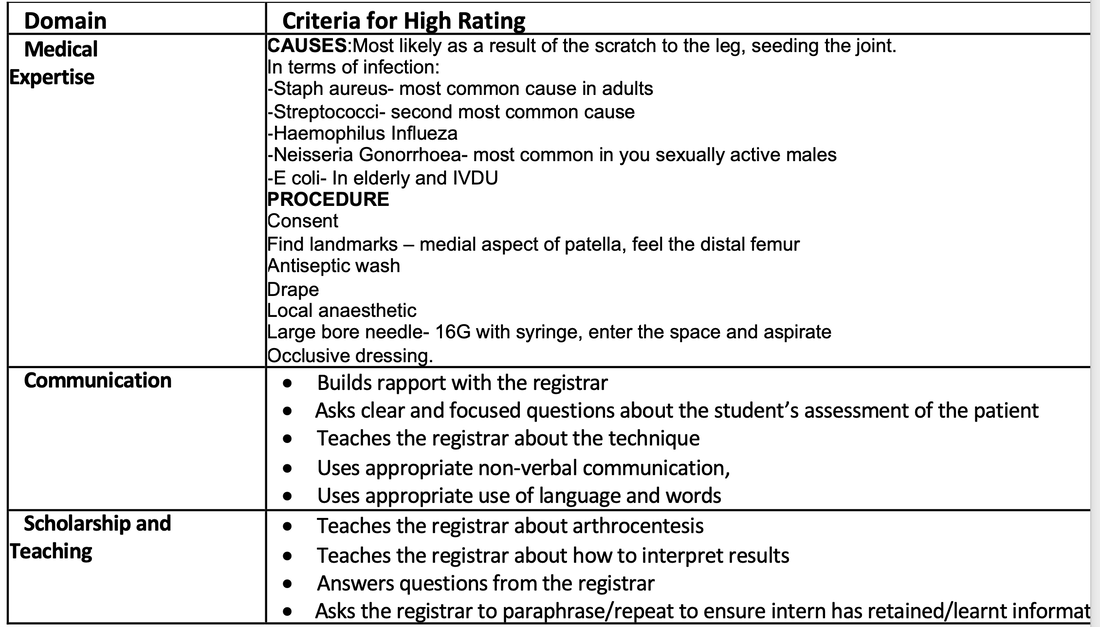
The patient, a 40 year old man has presented with a right sided knee effusion and very red and tender knee.
The patient is currently stable under the care of a senior registrar who has performed a knee joint aspiration prior to you arriving. Some results have returned:
KNEE ASPIRATE
Appearance: Yellow/Cloudy
WCC 62000/mcL
PMN% 66%
Crystals: Present, Birefringent
Your tasks are to:
This OSCE will assess the following domains:
You are at your tertiary referral hospital, it is 11 am on a Wednesday.
The patient, a 40 year old man has presented with a right sided knee effusion and very red and tender knee.
The patient is currently stable under the care of a senior registrar who has performed a knee joint aspiration prior to you arriving. Some results have returned:
KNEE ASPIRATE
Appearance: Yellow/Cloudy
WCC 62000/mcL
PMN% 66%
Crystals: Present, Birefringent
Your tasks are to:
- Outline a brief differential diagnosis (10%)
- Outline the procedure of a knee joint aspiration (60%)
- Interpret the results shown above (30%)
This OSCE will assess the following domains:
- Medical Expertise
- Communication
ANSWER
QUESTION 3 + ANSWER
CANDIDATE INSTRUCTIONS
You are working in a tertiary referral centre, it is 11 am on a Wednesday.
The patient, who is currently in Resus, presented following a syncopal episode without head injury. He has no other past medical history and is on no medications. John describes having had a previous episode of syncope, for which he did not seek medical attention.
The patient is currently stable in the resuscitation room under the care of a senior registrar and therefore you have time and/or several minutes to discuss this case.
You are not required to take a further history. Management is not a focus of this OSCE.
Your tasks are to:
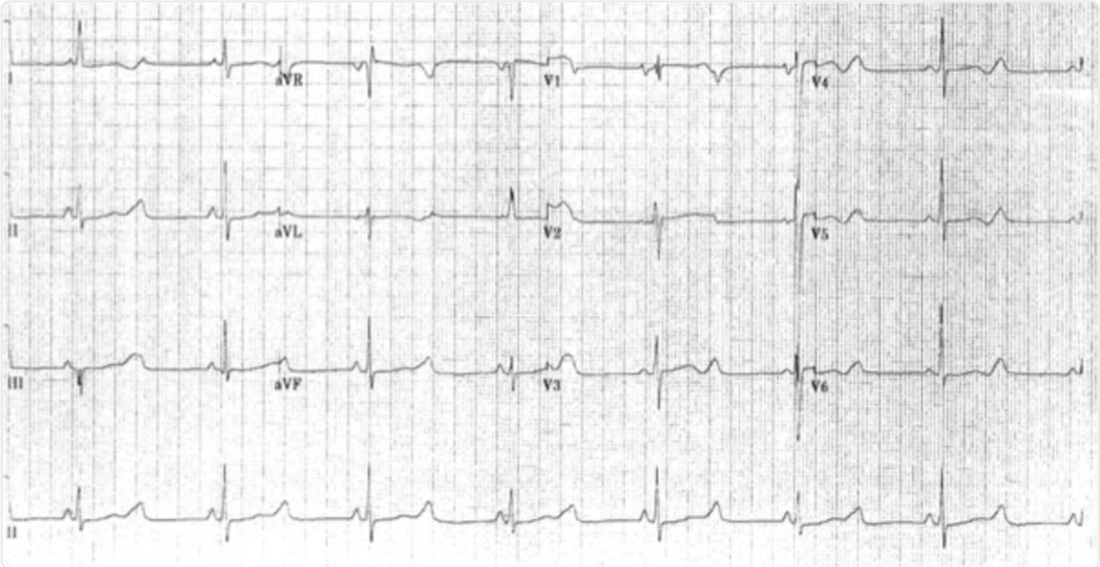
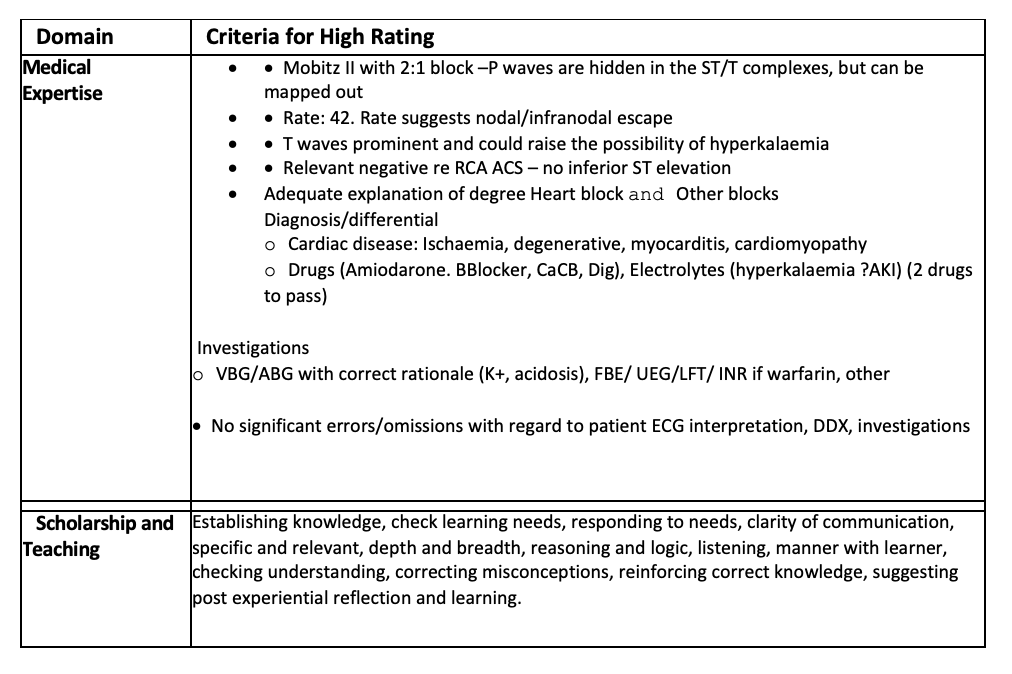
· Interpret the ECG (60%)
· Discuss the potential causes for the patient’s presentation (20%)
· Explain what investigations would be required (20%)
This OSCE will assess the following domains:
· Medical Expertise
· Communication
You are working in a tertiary referral centre, it is 11 am on a Wednesday.
The patient, who is currently in Resus, presented following a syncopal episode without head injury. He has no other past medical history and is on no medications. John describes having had a previous episode of syncope, for which he did not seek medical attention.
The patient is currently stable in the resuscitation room under the care of a senior registrar and therefore you have time and/or several minutes to discuss this case.
You are not required to take a further history. Management is not a focus of this OSCE.
Your tasks are to:
· Interpret the ECG (60%)
· Discuss the potential causes for the patient’s presentation (20%)
· Explain what investigations would be required (20%)
This OSCE will assess the following domains:
· Medical Expertise
· Communication
QUESTION 4 + ANSWER
Candidate Instructions
You are the duty consultant in a busy suburban emergency department. It is a Monday afternoon. One of your registrars approaches you to discuss a case. The patient is 65 year old man who is otherwise fit and well with a distant history of smoking in his youth. He has presented with central/R sided chest pain and SOB. He has been unwell for 4 days with pain worse on inspiration. He had flown from Sydney to Melbourne a week before.
On arrival his observations were:
Pulse 115/min reg, BP 125/70, sats 92% RA, RR24. Temp 37.9oC
His chest is reportedly clear on auscultation. He has no calf tenderness.
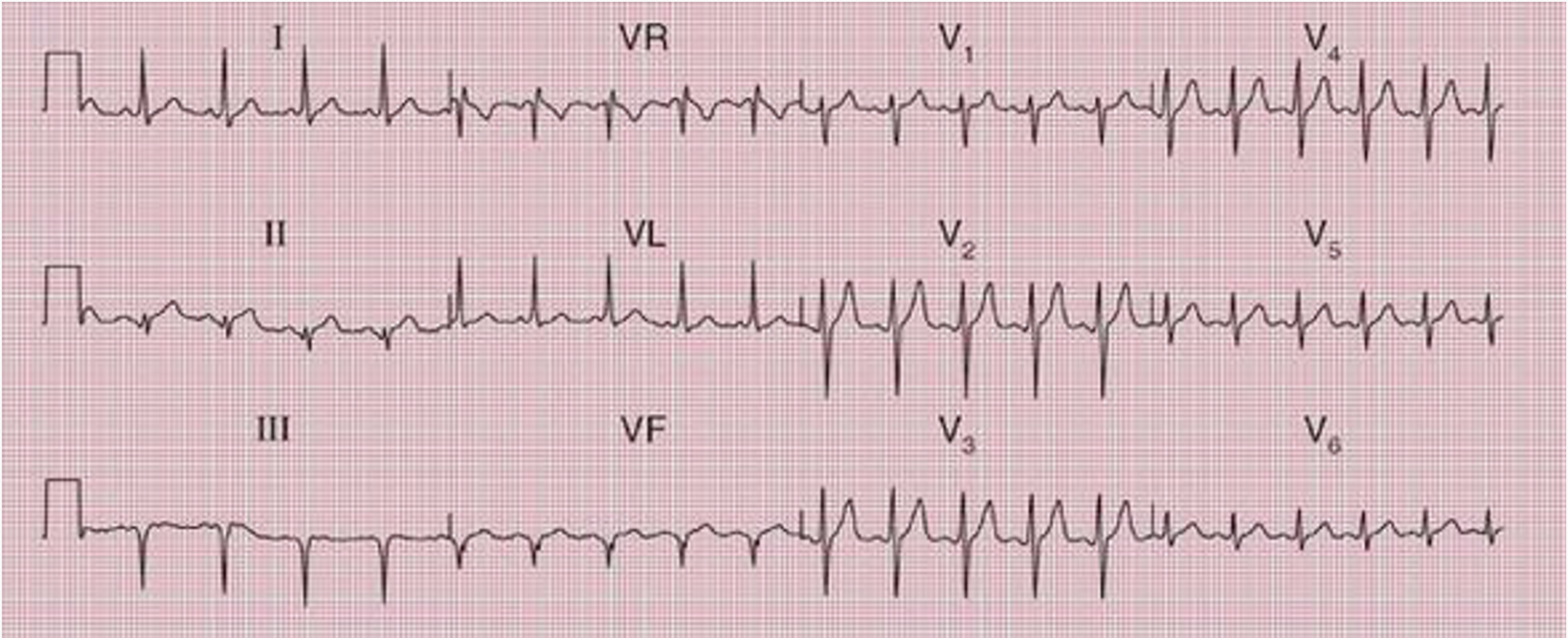
His ECG is shown below
You are the duty consultant in a busy suburban emergency department. It is a Monday afternoon. One of your registrars approaches you to discuss a case. The patient is 65 year old man who is otherwise fit and well with a distant history of smoking in his youth. He has presented with central/R sided chest pain and SOB. He has been unwell for 4 days with pain worse on inspiration. He had flown from Sydney to Melbourne a week before.
On arrival his observations were:
Pulse 115/min reg, BP 125/70, sats 92% RA, RR24. Temp 37.9oC
His chest is reportedly clear on auscultation. He has no calf tenderness.
His ECG is shown below
Labs include an ABG:
pH 7.28
PO2 68
PCO2 40
HCO3 18
BE -6
Na 141
K 4.6
Cl- 106
Gluc 5.8
Troponin was 10ng/L (normal range <14ng/L)
Creatinine 160mmol/l (normal <110)
Urea 7.6mmol/L (normal 2.5-7.1mmol/L)
D Dimer was 0.7mg/L (Normal range <0.5mg/L)
You will be assessed on the following tasks:
Medical Expertise
Communication
pH 7.28
PO2 68
PCO2 40
HCO3 18
BE -6
Na 141
K 4.6
Cl- 106
Gluc 5.8
Troponin was 10ng/L (normal range <14ng/L)
Creatinine 160mmol/l (normal <110)
Urea 7.6mmol/L (normal 2.5-7.1mmol/L)
D Dimer was 0.7mg/L (Normal range <0.5mg/L)
You will be assessed on the following tasks:
- Give a brief differential diagnosis (10%)
- Define massive and submassive pulmonary embolism (10%)
- Outline your approach to diagnosing Pulmonary Embolism (80%)
Medical Expertise
Communication
ANSWER
We covered the answer to this at length during the Viva.
Must cover the ECG and VBG in the answer, plus discuss the other blood results, including troponin.
Simple DDx ( the top 3 count)
Define massive vs submissive PE
Massive PE= acute PE with SBP <90 mmHg.
Submassive PE= acute PE without systemic hypotension but may have either RV dysfunction or myocardial necrosis(raised troponin)
Approach to diagnosis:
History and Examination
In history assessing the risk
We covered the answer to this at length during the Viva.
Must cover the ECG and VBG in the answer, plus discuss the other blood results, including troponin.
Simple DDx ( the top 3 count)
- PE
- ACS
- Pneumonia
- Pneumothorax
- Pericardial collection
Define massive vs submissive PE
Massive PE= acute PE with SBP <90 mmHg.
Submassive PE= acute PE without systemic hypotension but may have either RV dysfunction or myocardial necrosis(raised troponin)
Approach to diagnosis:
History and Examination
In history assessing the risk
- apply scores: PERC No, Wells Yes
- Investigations: Bedside, Labs(discuss D-dimer) Imaging(CTPA vs V/Q)
QUESTION 5 + ANSWER
Candidate Information
You are the duty consultant of a Regional Base Hospital Emergency Department.
A 32 year old woman, who is 32 weeks gestation is brought in by ambulance. She has been involved in a high speed motor vehicle accident. She has sustained a head injury with a small scalp laceration. She complains of right sided chest wall tenderness on palpation and has a painful right knee, with no obvious other injury.
On arrival the patient is conscious and alert and in a hard, cervical collar. The ambulance officers state that the patients GCS has always been 15 and blood glucose was 5.5. The ambulance have established intravenous access, and given Fentanyl for analgesia. On arrival the patient’s vitals are as follows:
HR 92 bpm
BP 110/40 mmHg
Sats 97% on 6L
RR 26
Her examination is demonstates a 2cm scalp laceration over the vertex of the skull. She has a painful right chest wall to palpation. The right knee is painful, but can be moved through a full range of motion. There is no neck pain and there are no focal neurological deficits.
Past history includes gastro-oesophageal reflux.
You will be assessed on the following:
Domains to be examined:
You are the duty consultant of a Regional Base Hospital Emergency Department.
A 32 year old woman, who is 32 weeks gestation is brought in by ambulance. She has been involved in a high speed motor vehicle accident. She has sustained a head injury with a small scalp laceration. She complains of right sided chest wall tenderness on palpation and has a painful right knee, with no obvious other injury.
On arrival the patient is conscious and alert and in a hard, cervical collar. The ambulance officers state that the patients GCS has always been 15 and blood glucose was 5.5. The ambulance have established intravenous access, and given Fentanyl for analgesia. On arrival the patient’s vitals are as follows:
HR 92 bpm
BP 110/40 mmHg
Sats 97% on 6L
RR 26
Her examination is demonstates a 2cm scalp laceration over the vertex of the skull. She has a painful right chest wall to palpation. The right knee is painful, but can be moved through a full range of motion. There is no neck pain and there are no focal neurological deficits.
Past history includes gastro-oesophageal reflux.
You will be assessed on the following:
- How would you approach clearing this patient’s cervical spine? (10%)
- You decide to perform a chest X-ray and discuss performing a CT cervical spine with patient. The patient is concerned about radiation exposure to the fetus. Please explain the potential exposure and what this means (70%)
- What are the potential injuries you are concerned about in blunt trauma in pregnancy? (15%)
- How would you prioritise this patients definitive management?(5%)
Domains to be examined:
- Medical Expertise (80%)
- Prioritisation and Decision-making (20%)
ANSWER
Standardised Case-Based Discussion (SCBD): Candidate Expectations
Part 1
How would you approach clearing this patient’s cervical spine?
Part 2
You decide to perform a chest Xray and discuss performing a CT cervical spine with patient.
The patient is concerned about radiation exposure to the fetus.
Part 3
What are the potential injuries you are concerned about in blunt trauma in pregnancy?
Placental abruption
Most common cause of fetal death in blunt trauma
May occur after minor injury
Most occur in the first few hours
Almost all occur in the first 24 hours
May have vaginal bleeding
Need a CTG
Placental rupture
Rare
100% fetal mortality
Fetal injury
Rare in blunt trauma. Usually due to skull fracture in maternal pelvic fracture
Prioritisation and decision-making
o Explain why normal vitals are misleading in the trauma patient
o Justify decision to perform an xray
o Explain and justify the need for right sided tilt
o Prioritise urgent transfer to a tertiary ICU which can deliver 3rd line care as needed
Standardised Case-Based Discussion (SCBD): Candidate Expectations
Part 1
How would you approach clearing this patient’s cervical spine?
Part 2
You decide to perform a chest Xray and discuss performing a CT cervical spine with patient.
The patient is concerned about radiation exposure to the fetus.
Part 3
What are the potential injuries you are concerned about in blunt trauma in pregnancy?
Placental abruption
Most common cause of fetal death in blunt trauma
May occur after minor injury
Most occur in the first few hours
Almost all occur in the first 24 hours
May have vaginal bleeding
Need a CTG
Placental rupture
Rare
100% fetal mortality
Fetal injury
Rare in blunt trauma. Usually due to skull fracture in maternal pelvic fracture
Prioritisation and decision-making
o Explain why normal vitals are misleading in the trauma patient
o Justify decision to perform an xray
o Explain and justify the need for right sided tilt
o Prioritise urgent transfer to a tertiary ICU which can deliver 3rd line care as needed
Next VIVA Meeting Monday 1st August 1830pm Melbourne time.
Don't forget your paediatric homework, preparing topics.
Don't forget your paediatric homework, preparing topics.